So, you’re on a bouldering trip. You’re trying to send your project and you jump for the last hold only to miss and come crashing into the pads. Only this time instead of shouting in frustration and then resting up for another go your ankle rolls and you’re immediately in lots of pain.
Ankle sprains are all too common in climbers and unlike overuse injuries only so much can be done to avoid them. However, if you do sprain an ankle the best thing you can do is rehab it properly so that you can get back to climbing as quickly as possible.
Today we have an article written for TrainingBeta by chiropractor and sport injury rehabilitation specialist Natasha Barnes in which she outlines her protocol for diagnosing and then rehabbing ankle sprains.
Natasha Barnes on Ankle Sprains
Ankle sprains are one of the most common injuries among climbers following finger, shoulder and elbow injuries. Here is how I approach the initial treatment of an acute ankle sprain.
DO YOU NEED IMAGING?
Although most patients with ankle sprains who present to emergency departments undergo radiography, less than 15% have a fracture.
My suspicion is that this number is slightly higher in climbers due to the fact that most sustain ankle sprains during a fall from a significant height rather than on field or during normal walking or running activities, but this is just speculation.
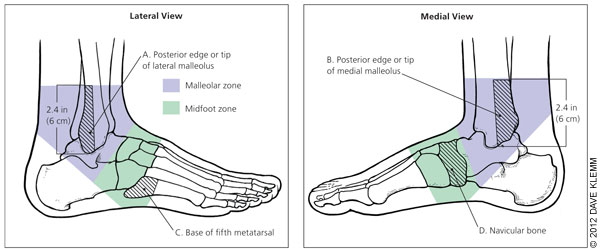
Ankle sprains should be evaluated using the Ottawa ankle rules, which are well-established clinical guidelines used to determine the need for radiography.
According to the Ottawa ankle rules, ankle radiography is needed if any of the following are true:
-
There is pain in the malleolar zone, plus either bone tenderness over areas of potential fracture which are the posterior edge or tip of the lateral or medial malleolus.
-
An inability to bear weight for four steps immediately after the injury and in the emergency department or physician’s office.
-
If there is pain in the midfoot zone, plus either bone tenderness over areas of potential fracture which are the base of the fifth metatarsal or the navicular bone of the midfoot.
Multiple studies have demonstrated that the Ottawa ankle rules are nearly 100 percent sensitive for detecting fractures in adults and children as young as five years. Therefore, negative findings eliminate the need for radiography. However, because specificity is low (30 to 50 percent), positive findings do not necessarily indicate that a fracture is present, but do indicate that radiography is needed to confirm or rule out fracture.
If you have any of the above positive findings according to the Ottawa ankle rules seek medical attention immediately and get imaging to rule out fracture.
*Disclaimer: This post is not intended to be a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition. Never disregard professional medical advice or delay in seeking it because of something you have read online.
Ok, I don’t have a fracture. What next?
DON’T ICE THAT ANKLE SPRAIN!!!
According to a 2012 study in the British Journal of Sports Medicine, ice is commonly used after acute muscle strains, but there are no clinical studies of its effectiveness. Some studies say icing could be counterproductive in the long run because it seems not to improve but, rather, delay recovery from eccentric exercise-induced muscle damage.
Inflammation is normal and beneficial to the healing process. You must allow the inflammatory process to take place. Don’t hinder it with icing.
Ice can relieve pain but will cause a congestion of the tissue. It causes a backflow of the interstitial space, shuts off the signal between the muscles and nerves, and does not help the evacuation of deoxygenated blood and waste. Therefore, ice is counterproductive!
Ibuprofen is worse because it actually stops the signal of the inflammatory response, not just prevents it. The body’s natural inflammatory response is not a mistake!
Here is a great article listing 10 reasons icing injuries is wrong.
http://stoneathleticmedicine.
WHAT SHOULD I DO IF I DON’T ICE?!
Traction, movement and heat!
Traction will release the pressure and movement will encourage blood flow to the area which is rich with healing factors such as oxygen and white and red blood cells. The key is blood flow. If you want something to heal, it requires blood!
In addition, movement with traction reduces pain, enhances lymphatic removal of inflammation, improves flexibility, and restores normal joint alignment. The waste products are evacuated through the lymphatic system, not the circulatory system (the particles are too big). Therefore, muscle contraction via movement is necessary to move lymph and eliminate these chemicals, not immobilization!
Here are a few things you can do to get some traction and movement all at once with a little bit of compression to squeeze out some of the acute swelling.
Active range of motion with a voodoo band
Wrap a voodoo compression band starting midfoot working up over the ankle, then move the ankle thru its full range. This can be done actively by pointing your toes and then bring the back up as far as you can.

Resisted plantar flexion and dorsiflexion with traction
Loop a stretch band around the forefoot while the voodoo band is on to resist plantar flexion (pointing foot down) and hold onto the ends. Use another stretch band wrapped around the foot pulling the other direction to traction the ankle and resist the foot and toes in dorsiflexion (pointing foot towards you). Move ankle in plantar and dorsiflexion or in circles clockwise and counterclockwise Aim for 10-20 reps and 3-4 sets with a short rest in between.


Elevated dorsiflexion mobilization
Elevated dorsiflexion mobilization can be helpful as well for increasing dorsiflexion which typically gets restricted with an ankle sprain. This works with the voodoo floss wrapped around the ankle or with a stretch band looped around the lowest part of the ankle pulling posteriorly.
Here is how to perform it:
Place the involved foot on a plyo box or bench. Lean forward tracking the knee directly over the foot as far as possible while keeping the heel planted. A stick or PVC pipe can be used for balance. Repeat several times before taking the band off.



Light goblet squats with voodoo band
Hold a kettlebell at chest level. Stand with feet shoulder width apart with slight turn out in your toes (about 15° of turn out). Squat down to just below parallel with your thighs with knees tracking out over toes. Perform 10-20 reps for 3-4 sets.
Let pain be your guide on this exercise. Not everyone can handle this one with a fresh ankle sprain. If it’s more painful than a 2-3 out of 10 then hold off on this for a week or two.


Putting It All Together
There is a little more involved in fully rehabbing an ankle sprain than these exercises (although soft tissue work and more general/specific strengthening can be done for example). These are just some of the strategies that I use to get over the hump on an acute ankle sprain. These strategies can work very well on an old ankle sprain that did not heal properly too!
Hope these are helpful and I hope you enjoyed the article! If you are in San Francisco and have a climbing related injury come visit me at Motus Clinic and we can develop a strategy for helping you get over your injury. Book online HERE.
References
-
Bachmann LM, Kolb E, Koller MT, Steurer J, ter Riet G. Accuracy of Ottawa ankle rules to exclude fractures of the ankle and mid-foot: systematic review. BMJ. 2003;326(7386):417.
-
Stiell, I. G. (1993). Decision rules for the use of radiography in acute ankle injuries. Refinement and prospective validation. JAMA: The Journal of the American Medical Association,269(9), 1127-1132. doi:10.1001/jama.269.9.1127
-
Ivins D. Acute ankle sprain: an update. Am Fam Physician. 2006;74(10):1719.
-
Hubbard TJ, Denegar CR. Does cryotherapy improve outcomes with soft tissue injury? J Athl Train. 2004;39(3):278–279.
-
Bleakley, C. M., Glasgow, P., & Webb, M. J. (2011). Cooling an acute muscle injury: can basic scientific theory translate into the clinical setting? British Journal of Sports Medicine,46(4), 296-298. doi:10.1136/bjsm.2011.086116
-
Tseng, C., Lee, J., Tsai, Y., Lee, S., Kao, C., Liu, T., . . . Kuo, C. (2013). Topical Cooling (Icing) Delays Recovery From Eccentric Exercise–Induced Muscle Damage. Journal of Strength and Conditioning Research,27(5), 1354-1361. doi:10.1519/jsc.
0b013e318267a22c -
Bekerom, M. P., Struijs, P. A., Blankevoort, L., Welling, L., Dijk, C. N., & Kerkhoffs, G. M. (2012). What Is the Evidence for Rest, Ice, Compression, and Elevation Therapy in the Treatment of Ankle Sprains in Adults? Journal of Athletic Training,47(4), 435-443. doi:10.4085/1062-6050-47.4.14
Cover Photo: courtesy of Stephanie Hsie | @mineralpursuits
About The Author

Natasha Barnes is a former competitive climber, a competitive power lifter, and a doctor of chiropractic with a specialty in rehabilitation of sports injuries. She lives in San Francisco, California and has a private practice at Motus Clinic.
She graduated from a 4-year graduate program at Palmer West Chiropractic School in San Jose, CA in 2012 with a specialty in sports medicine and physiotherapy. She’s a ClinicalAthlete provider for San Francisco, certified in Functional Range Release Technique (upper limb) and Myofascial Decompression (cup therapy).


You crazy if you think I’m going to wrap my swollen hurt ankle in super tight rubber and move it. I can barely get it to flex it’s normal movement on its own
I’ve sprained my ankle lightly (fell off the pavement when jogging)
When do you recommend is a good time to go back to weightlifting?
Thank you very much