
Jared Vagy on Healing Elbow Injuries in Climbers
Date: August 12th, 2019
Dr. Jared Vagy is a physical therapist, and he’s a climber who’s incredibly motivated to help other climbers heal their bodies. In this interview, we talk about how to heal common elbow injuries in climbers. It’s super in-depth and he describes exact protocols to use on elbow injuries, so I hope it helps you out.
Other Interviews with Jared
- In my first interview with Dr. Vagy on the podcast we talked in general about how to heal injuries, but since that time he has gotten way more specific about the steps we need to take to address them.
- In our second interview he talked about how to heal shoulder impingement.
- In our third interview, we talked about rotator cuff injuries and neck strain.
- In our fourth interview, we discussed finger pulley sprains.
Jared also wrote a paperback book all about healing climbing injuries called Climb Injury-Free. In it, he describes his 4-step pyramid to healing injuries:

In the book he discusses injuries of all kinds, but in this interview we focus on inside elbow pain, outside elbow pain, and how to heal them.
Jared just released 2 new Elbow Pain protocols on TrainingBeta last week:
Here are his other four protocols:
You can see a description of all of the protocols (which we’ve made available for $10 each) at www.trainingbeta.com/rock-rehab.
Jared Vagy Professional Credentials
Dr. Vagy is an authority on climbing related injuries. He has published numerous articles on injury prevention and delivers lectures and seminars on the topic. He received his Doctorate in Physical Therapy (DPT) from the University of Southern California, ranked the number one DPT Program in the nation for the last decade by US News and World Report. He is now a professor at the University in the DPT Program. As a Doctor of Physical Therapy in clinical practice, he went on to complete a one year residency program in orthopedics and a one year fellowship program in movement science. He is a Board Certified Orthopedic Clinical Specialist and a Certified Strength and Conditioning Specialist.
Dr. Jared Vagy Interview Details
- How elbow injuries happen
- What the different elbow injuries are
- How to figure out what injury you have
- When to start climbing again
- How to heal the elbow injury
- How to avoid elbow injuries in the future
Supporting Documents from Podcast
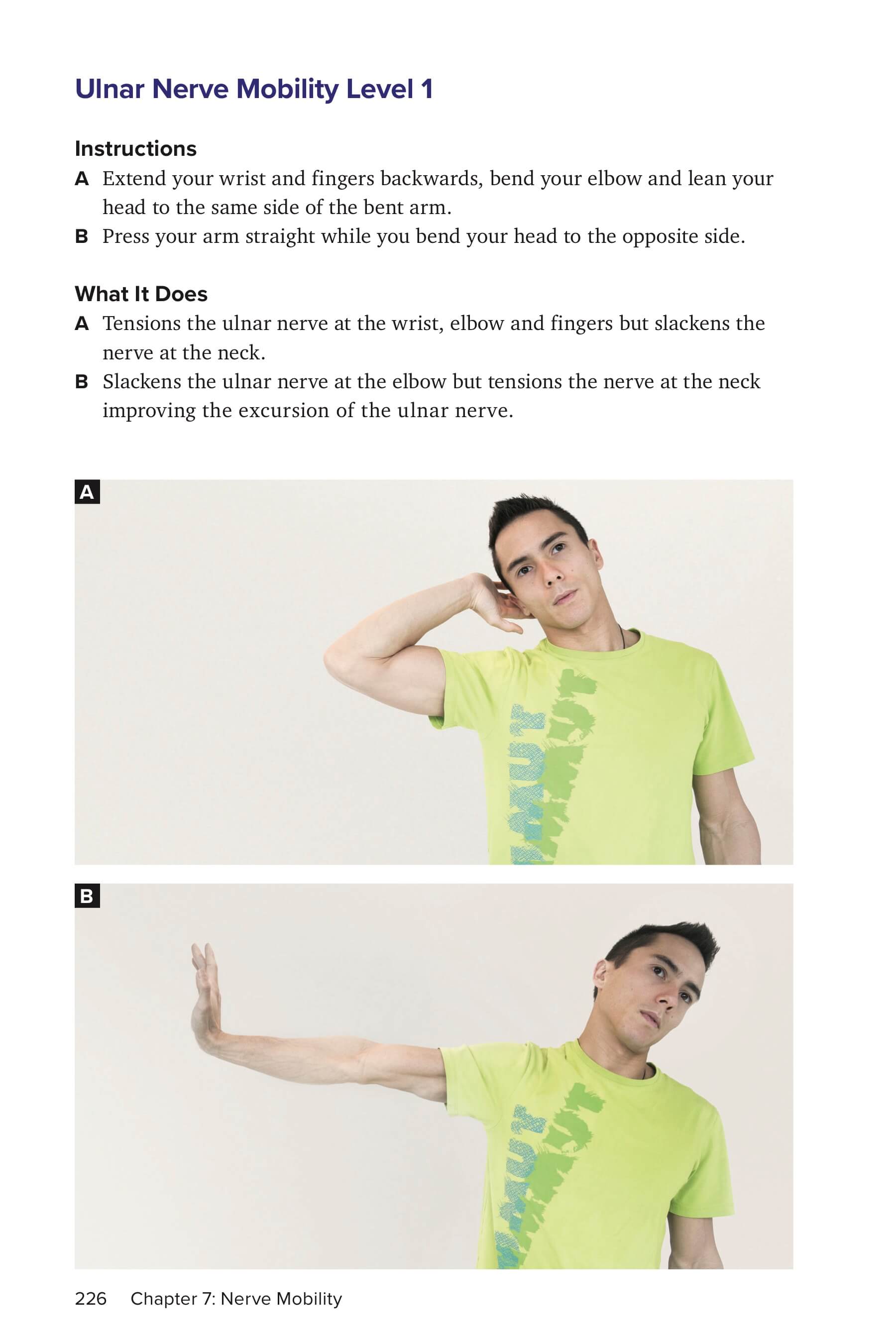
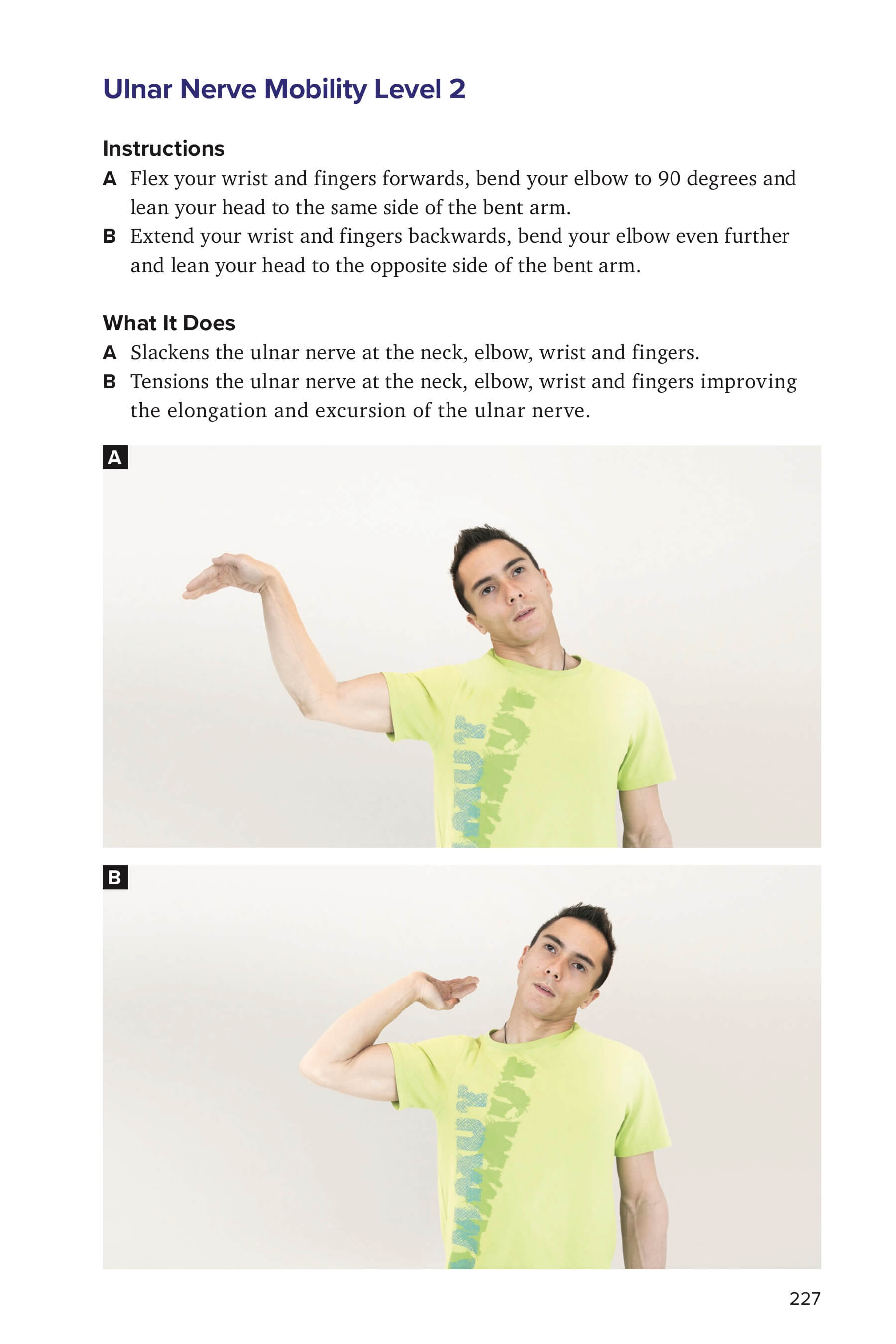
- Ulnar Nerve Mobility Exercise Level 1 and Level 2
- Video of proper elbow form while climbing a warm-up
- Video of proper elbow form while climbing a harder boulder
- Cupping tools he uses
{kind=link}
{kind=link}
Rock Rehab Protocol Links
- Inside Elbow Pain
- Outside Elbow Pain
- Finger Pulley Sprain
- Shoulder Impingement
- Rotator Cuff Strain
- Neck Strain
- Jared’s book, Climb Injury Free
- Website: www.theclimbingdoctor.com
- Instagram: @theclimbingdoctor
Training Programs for You
Do you want a well-laid-out, easy-to-follow training program that will get you stronger quickly? Here’s what we have to offer on TrainingBeta. Something for everyone…
- Personal Training Online: www.trainingbeta.com/mercedes
- For Boulderers: Bouldering Training Program for boulderers of all abilities
- For Route Climbers: Route Climbing Training Program for route climbers of all abilities
- Finger Strength : www.trainingbeta.com/fingers
- All of our training programs: Training Programs Page

Please Review The Podcast on iTunes
Please give the podcast an honest review on iTunes here to help the show reach more curious climbers around the world.
Transcript
Neely Quinn: Welcome to the TrainingBeta podcast where I talk with climbers and trainers about how we can get a little better at our favorite sport. I’m your host, Neely Quinn, and I want to remind you that the TrainingBeta podcast is an offshoot of a site that I created called trainingbeta.com. It’s all about training for climbing.
Over there we have regular blog posts, we have climbing training programs for all different levels and all types of climbing, we have nutrition coaching with myself – I’m a nutritionist – and we also have online personal training with Matt Pincus.
You can go to trainingbeta.com and find out more about all those services and hopefully one or more of them will make you a better climber.
Welcome to episode 130 of the podcast. I’m really sorry I didn’t get an episode out in the last couple weeks. I’m trying to climb during the week now, like on Wednesday-Thursday. Part of the reason that I created TrainingBeta in the first place was so that I could be my own boss and have my own schedule so that I could climb during the week when it’s less busy and crowded at crags. I’m finally getting to do that with my friend, Paige Claassen. We’re both working on hard projects for ourselves during the week now and trying to balance that with working and podcasting and seeing clients and also climbing and training on the weekends. I’m trying to figure it out. I’m doing my best and I’ll try to get a podcast out once every other week for the remainder of the summer. Hopefully I can get my stuff together enough to do that.
Anyways, today I am talking with Jared Vagy. Jared is a physical therapist. He’s out of California. He’s also a professor of physical therapy and he’s a climber so he’s a really, really good resource for us as climbers. He’s been on the show quite a few times before talking about other body parts. Today we’re talking about elbows.
Jared also created these protocols for each of the really common body parts that climbers hurt. He called it the Rock Rehab Pyramid. He talks about how to get an injury out of the super inflamed acute stage and how to then rehab it back to normal strength and also how to prehab things, like how to avoid injuries. If you go to trainingbeta.com/rock-rehab, or just go to the ‘Programs’ page and scroll down, you’ll find Jared’s stuff in there. He’s got one on neck strain, shoulder impingement, rotator cuff strain, pulley strain for your fingers, and now we’re adding the elbows. There are two protocols in there now, one for inside pain in your elbows and one for outside pain.
Elbows are obviously a very common injury for climbers so today we’re going to talk about: what are the common injuries, how to know what you have, and how to make it stop hurting. Hopefully this will help you and I’ll just let Jared take it from here. Here’s Jared Vagy. Enjoy and I’ll talk to you on the other side.
Neely Quinn: Welcome back to the podcast Jared. Thanks very much for talking with me today.
Dr. Jared Vagy: Excellent. I’m excited to be on.
Neely Quinn: Cool. Anything new in your world to update us on?
Dr. Jared Vagy: I mean, there’s always new things but I’ve just been keeping busy. I relate it to I now have to schedule things in 15-minute increments. It used to be I’d be like, ‘Oh yeah! Let’s go ahead and schedule this at 4:00PM or noon,’ and now I’m like, ‘Alright, at 3:15-3:45 let’s have this discussion,’ or this talk. Things have been just a little bit crazy.
Earlier, right before we started this, I was teaching online in the doctoral physical therapy program at USC then we have this podcast, which I’ve been psyched to do, and then I have a 10-minute window to jump on a ride share and head over to Vegas to get my butt kicked on some offwidth cracks.
Neely Quinn: You’re going to do some 15-minute increments on some offwidths?
Dr. Jared Vagy: Yeah, more like 15 minutes of going a couple inches and dry heaving and then keep going, but I’m excited. I’m meeting my longtime climbing partner. We’ve done a bunch of walls together and we’re reuniting and he’s going to get my butt kicked on some Las Vegas obscure Red Rock offwidths so we’ll see how that goes.
Neely Quinn: That’s cool. I’m happy to hear that you’re going to do something for fun. I mean, I know your work is fun for you but I’m glad you’re going out climbing. Good for you, Jared.
Dr. Jared Vagy: It’s been such a balance. This past calendar year I’ve been so busy professionally that I said, “You know what? Climbing is such a huge part of my life. I need to make this a big priority of just getting more time outside and even just getting more time in the gym, just training.” The past calendar year, at least for me, has been a huge push of saying, “Alright, this is going to be my big priority to stay fit and to get after some of my objectives and to really do what continues to drive me.”
I’m psyched in everything I do so it’s this constant trade-off of trying to balance everything with work and with life and with working with climbers as well. I’ve got to just keep climbing as much as possible so it’s been fun.
Neely Quinn: Have you finished any objectives or been psyched on your climbing?
Dr. Jared Vagy: I’ve been training and I have a couple things in mind this summer in Yosemite but mostly it’s been just trying to get as much outdoor time as possible. For me, bigger objectives and not necessarily the challenge of the route but the challenge of the entire experience of doing big walls has always been a passion of mine so really right now it’s just logging the hours, logging the time, and just getting outside and getting as much climbing in as I can do.
I was in South Africa, actually, last week which was pretty cool. I got to do some routes on Table Mountain which was some pretty epic scenery. I’ve been getting around a little bit and enjoying it.
Neely Quinn: Woah! You were in South Africa for work? Or just for climbing?
Dr. Jared Vagy: No, I took a trip. Almost all of my travel this past four years, the majority of it, has been for work. I’m either teaching a conference or teaching a seminar or working with a sports team overseas. I said, “You know what? I just need to take a trip for myself.” I just went to Africa and had some good experiences over there and got in some climbing and now I’m back in action, back in Los Angeles.
Neely Quinn: Nice! This is so great to hear. Good for you!
So, what are we talking about today?
Dr. Jared Vagy: We’re talking about elbows.
Neely Quinn: You said you were psyched for this podcast. Tell me why you are so excited about talking about elbows.
Dr. Jared Vagy: Neely, I’m psyched for every podcast that we have. I mean, I love talking about climbing and climber injuries and I love dorking out about it. Specifically the elbows, I think of them almost as a dumb joint or a dumb area of the body. Whatever happens at the elbows is kind of dictated by what the fingers and the wrists do – so how you apply your grip on the hold – and what our shoulder does and also the midsection.
I want to talk about elbows and actually talk through some patient cases I’ve had, so climbers or clients that have come in that have had elbow pain and what some common elbow injuries are. Then, the diagnostic process I go through to say, “Huh. This is a little bit different. Is there something else that’s going on?”
There are a couple key areas that climbers have pain in their elbows. There are four regions: the inside of the elbow which is the medial elbow, the outside which is the lateral, then the front and back, the anterior and posterior. I want to definitely talk through a couple of different patient cases and ways that I treat and different climbing movements that can predispose climbers to these types of injuries.
Neely Quinn: Okay. I’m excited. I have so many friends right now who have elbow issues and I know it’s super common. It seems to be one of those really stubborn injuries. Is that your experience with them?
Dr. Jared Vagy: It’s extremely stubborn. They’re the ones where I typically see clients or climbers after they’ve seen a couple physios or they’ve gone through some bouts of seeing medical professionals and these are the ones that linger. A lot of them are also misdiagnosed and I think that’s a reason why as well.
We’ll talk about what oftentimes causes the different locations of elbow pain. That’s one thing, but also there’s several additional layers that I want to bring up in this podcast that aren’t commonly addressed that can sometimes take that lingering – that 4-6 months or that 6-8 months of having pain in one location – and cut that down to quite a bit less time. I want to make sure we talk about those treatments and different ways to assess those on this podcast because a lot of people that have constant elbow pain sometimes are mismanaged. They’re just doing eccentric exercises or just doing a certain type of exercise but there’s a lot more going on at the elbow that I want to be able to talk about.
Neely Quinn: I’m very excited to hear about that part of this talk so let’s get started. Where do you want to start?
Dr. Jared Vagy: Let’s start with inside elbow pain or ‘medial elbow pain.’ What this is is if you look down at your elbow and you extend your arm outwards and you look at your forearm muscles and you trace them from your wrist down to the inside of your elbow, oftentimes climbers that have inside elbow pain have pain in this area. If you look it up online it’s called golfer’s elbow or medial epicondylosis. Those are the common terms that you’ll find.
Neely Quinn: And they’re all the same thing.
Dr. Jared Vagy: Yeah. Golfer’s elbow is a general term or a layman’s term. Medial epicondylosis is a degeneration of the tendon as it goes from your wrist flexors – so the muscles that move your wrist forward – and inserts into the little bone on the inside of your elbow. Those are common terms.
You’ll also find medial epicondylitis but -itis means inflammation and really, if you have medial epicondylitis that’s only the first two weeks that you’re having symptoms, when you have the inflammation. I’ll typically refer to it as medial epicondylosis and oftentimes climbers will just call it inside elbow pain.
Neely Quinn: Okay, so where does that usually come from?
Dr. Jared Vagy: I always first think about movements on the rock wall. What movements start to overwork those muscles that attach from the wrist into the inside elbow? Neely, can you think just about in climbing, those muscles that flex our fingers and flex our wrists – any particular holds or grips that you think may cause more stress on that area?
Neely Quinn: I mean, maybe slopers or pinches?
Dr. Jared Vagy: Yeah. Slopers definitely because you’re flexing that wrist forward. That’s going to overactivate those wrist flexor muscles and they’re in a really tough position. It’s called a length-tension – a tough position to turn on and that can cause some stress. Slopers are ones that climbers that climb a lot of routes that involve slopers are predisposed to getting that inside elbow pain. Pinches as well. That uses some of the muscles. Even in crimp positions you’re using those muscles in the front of your fingers to grip so really the way that I look at is climbers that tend to just overgrip holds, regardless of the holds that they are using.
If you think about it, if you’re on the crux of a route you’re going to want to grip as hard as possible to hold on so you can transition to the next move. If you’re just climbing, you’re warming up or climbing easier routes, you don’t want to overgrip. You want to keep that softer grip. These are often patterns that I’ll look for in climbers from their movement to see, ‘Are they overusing slopers? Are they overgripping when they climb?’ to see if that leads to overuse of the muscles that flex the wrists or flex the fingers.
Neely Quinn: So that makes sense and then what kinds of things will they see with this? Or how can they know for sure that this is what they have?
Dr. Jared Vagy: This is oftentimes tough to diagnose because there’s one other muscle that crosses that area as well and it’s called the pronator teres, or the pronator. If you look at the front of your forearm that goes from the little bone on the inside of your elbow across your arm, just on the top part of it. That’s a muscle that basically does what’s called pronation. It takes your wrist and rotates it away from you.
Imagine that your arms are down at your side – no, let’s do this like you’re on a climbing wall. Let’s say you’re standing on a climbing wall and your shoulder is lifted so your elbow is in front of you and you’re standing and you rotate your palm away from you and into the rock. Does that make sense, Neely?
Neely Quinn: I think so. Away from me, outside of my body?
Dr. Jared Vagy: Almost like let’s say you’re standing and you bring both elbows up to the level of your shoulder. Your elbows are bent to 90°, your palms are now facing away from you or facing your back and you rotate them in towards the rock wall so you can actually grip holds. That motion of rotating your lower arm is called pronation and that’s another muscle that attaches to that same area that, if it’s overworked or overused, it can lead to some pain.
You really have these three muscles: the muscle group that flexes your wrist, the muscle group that flexes your fingers, then this muscle that rotates your wrist into what’s called pronation. They all attach in that same area.
First of all, climbers need to first determine if they have inside elbow pain. It’s related to the tendon. Which of those muscles is the culprit for generating that inside elbow pain? Whether it’s the ones that flex your fingers, flex your wrist, or rotate your lower arm.
Neely Quinn: So what does that require? Pushing on it as a test?
Dr. Jared Vagy: It’s quite straightforward. You basically flex your fingers and if that generates pain – well, before I get into that there’s three steps that you do. If it’s a contractile tissue that we’re talking about, such as a muscle or tendon, then all you do is you stretch it so you lengthen the tissue, you activate it so you contract the tissue, and then you press on it/you palpate it. You lengthen, you activate, and you press on it. If all three of those generate symptoms then you have a high likelihood that this is the affected structure.
For example, someone activates the muscles that flex their fingers by just pulling down on a hold and they get inside elbow pain. Then they stretch those muscles that flex their fingers. They stretch them back into extension and they get inside elbow pain. Then you press on the inside elbow and that generates their symptoms? There’s a high likelihood that finger flexors are what is causing that inside elbow pain. You can do the same with the wrist and you can do the same with the pronators that rotate your arm inwards, that kind of step-by-step process.
A lot of climbers have that. They have one of those three, two of those three, three of those three. They’re generating that inside elbow pain, that medial epicondylosis, but many of them don’t or they have something in addition to that that’s also causing the pain. That’s why I want to take you through a patient case I had recently that was fascinating of someone that actually had inside elbow pain, or medial epicondylosis, as a diagnosis. They did have that. They did have a positive test that I just talked about but there was something else that was generating all their pain. We were able to correct that by actually changing how they move and changing how they climb.
Neely Quinn: Okay, take us through that.
Dr. Jared Vagy: Okay. So this patient came in and they had inside elbow pain. I went through those tests I just talked about where you stretch the structure, you activate the structure, you palpate the structure. A few of those were positive but it was a mixed bag. Some of them were positive for the wrist, some were positive for the fingers, and some of them were also positive for rotation or that pronation. I said, “Something is not right.” They had seen another physical therapist, they had gone through 12 weeks of therapy, and they weren’t getting better at all. It was lingering. They still had this inside elbow pain.
What I did then was I put them in this position – Neely, when you were little did you every play owl eyes? Or even now if you play with kids. You take your finger and you make an OK sign and you flip it around, like you rotate your elbow up in the air, and you pretend like you’re an owl that has these interesting finger eyes. Do you know what I’m talking about?
Neely Quinn: Totally.
Dr. Jared Vagy: Ok, so for all you listeners that haven’t played owl eyes maybe you can Google what it looks like. I put the patient in this position where I basically rotated him into this owl eye position on one arm. I made the OK sign, I rotated his elbow upwards, and I put him in this position. This position brought on his inside elbow pain. The same exact pain, it brought it on and he said, “That’s what I feel when I climb.”
The next thing that I did is I had him move his head towards his arm. This was his right arm that was affected. He’s lying down on the table, he’s in this owl eye position with his elbow up and his pointer finger and his thumb around his eye, and I just had him move his head towards that right side.
Neely Quinn: You mean like his head turns as if he’s going to look at his arm? Or his whole head tilts?
Dr. Jared Vagy: His head tilts, so almost bringing that right ear to his right shoulder. Just a clean side bend is what we would call it, or a tilt. He’s in that position, he has his elbow pinned, I tilt his head, and his pain goes away.
Neely Quinn: Woah.
Dr. Jared Vagy: This is common. This is actually extremely common so anybody with inside elbow pain, or we’ll talk about outside elbow pain as well, actually try this and see if it changes it. This is normal dynamics of the body.
Then I tilted his head the opposite direction and what do you think happened to his pain? It’s the opposite of going away.
Neely Quinn: It came back. I’m trying to figure out why did it do that?
Dr. Jared Vagy: I know. Isn’t that crazy? I tilted it the opposite direction and his pain increased. I actually moved his head away from that arm and his pain increased. Like I said, this is a normal finding and I see this all the time. It gets missed quite a bit.
You were saying, Neely, that you wonder why it does that. Tell me what your thought process is because it doesn’t make sense, right?
Neely Quinn: I mean, it seems like it has something to do with the neck or nerves or something.
Dr. Jared Vagy: Exactly. His arm never changed position. His arm was in that same position but we moved his neck and his elbow pain changed. Really, what we’re doing with that is called neurodynamics. The nerves in our body that come out through our neck come down through the muscles in the neck, through the front of the chest, down into the upper arm, and then down into the lower arm and they pass through these series of interfaces through muscle and fascia.
Those nerves can actually glide and move, almost like the brakes on a bicycle. You know how you squeeze the brake on a bicycle and the wire moves within that sheath? That’s just like how nerves move in our body. If you can move someone’s neck and change pain in their elbow there isn’t a muscle that continuously goes from the elbow all the way to the neck so the only thing that we’re changing is neurovascular structures.
Imagine this rubber band comes out from the neck and goes all the way down and let’s say into the elbow in this case, and also into the wrist and fingers. You’re taking that rubber band and as they side bend, they bring that right ear to the right shoulder, the rubber band is put on slack. Like you’re climbing and you give your partner a little bit of slack with the rope. You bend your ear to the other side and now that rope or that nerve is put on tension, almost like you’re short-roping your climbing partner.
That’s a test that I’ll oftentimes have climbers do, especially with inside elbow pain or outside elbow pain, to differentiate whether it is truly these tendinopathies that we talked about earlier or if it’s really something else, like whether it’s just a nerve that’s getting aggravated and that is constantly generating pain.
Neely Quinn: So what does that mean? What did you guys do?
Dr. Jared Vagy: What’s the outcome? We went through a number of other tests and all these other tests came out fine. We identified that this was their symptom. This is what was kind of driving and generating.
The first thing I do is I watch their movement. I watch them climb. When I see clients I make it almost mandatory for them to either bring in climbing footage or for us to schedule something where I’m at a location to watch them move. There were two different clips and both of the clips was dead-on, every single movement he would do, he would do the exact same position of his elbow. He would grab the hold – these are positions that I had him go back for our second session and re-climb the same climbs and completely modified how he climbed them. He didn’t have to climb it this way.
Think of a slightly overhead gaston movement. You’re grabbing the hold and your elbow is in this upward position. Your wrist is cocked back a little bit, especially if it’s a little bit of a crimp, and that position is very similar – it’s not as aggressive but it’s very similar – to this owl eye position I told you about where you make this OK sign and you lift your elbow up. You now take that OK sign and you reach across your body and you’re grabbing a crimp or a hold. He would grip almost every hold – and he didn’t even realize this, this was from the footage – in this position that puts tension on what’s called the ulnar nerve. Every time he would grab a hold he would basically flare his elbow upward.
The movement that we modified is he went back to the climbing gym and he just relaxed his elbow down a little bit, kind of in line with gravity, as he would grasp the holds on the climbing route. I gave him a series of other things and we’ll talk about that in a moment for anyone that has this condition, but for that particular condition the thing that helped him the most was modifying how he moves on the wall by changing that constant, repetitive, high elbow position as he gripped.
Neely Quinn: Do you see a lot of people doing that in the gym?
Dr. Jared Vagy: It depends on the style of them as a climber. I can almost classify someone that climbs a lot with flexed and high elbows. You can pick those people out pretty frequently but then the ones that also get this injury are ones that don’t do that unless they’re on a crux move.
Yes, I could point that out quite a bit on people that are on a crux move. You know it. You feel it. You’re pushing really hard then you start to chicken wing upwards, right? That’s one where it was almost an example where I was like, ‘Wow. On an 8-move boulder problem 7 of the moves were high elbow? That’s not that common.’ That was this very isolated example but I see it so much on people that are cruxing out. When you’re cruxing out that’s usually when you’re going to get the most overuse injuries or make it hurt. It’s something that I see that’s pretty common. It’s a chicken wing but you’re especially a chicken winging when you’re reaching across your body in almost a higher gaston.
Neely Quinn: I mean, it would be super cool to see a photo or a video of this. I don’t suppose he would let you share his video.
Dr. Jared Vagy: Let me see what I can do. After this, let me take a note and let me see if I can get some clearance on that. If I am, awesome. Let me post it. If not, let me just put a video and a photo up that you can attach to the podcast that shows the position so people know what I’m talking about and they can identify it as they are moving themselves.
Neely Quinn: Yeah, that’d be awesome. That’d be great.
Dr. Jared Vagy: I’ll reach out after the podcast and see.
Then what you do is if we have a nerve issue we correct the movement, we change the movement, but how do we decompress the nerve? How can we take all that pressure from the muscles that are on top of the nerve and take that pressure off of them? Do you have any ideas of what you would do to the muscles – we’re perceiving that this nerve is being tensioned and the muscles are also compressing on the top of them – how to decompress the muscles?
Neely Quinn: I’ve had things like this and acupuncture has helped or super deep tissue massage so I’m assuming just relaxing the muscle a little bit.
Dr. Jared Vagy: Relaxing the muscle is quite important but what I found, and this happens in climbers with a lot of inside elbow pain, if it’s in addition related to the nerve, that deep pressure is actually pushing the muscle on top of the nerve. Does that make sense? The nerve is right under the muscle and as you press into the muscle it feels good and you’re releasing this stiffness but you’re also compressing the muscular tissue onto the nerve and that can cause some irritation as well.
In this particular case, if you having something that’s affected with your nerve then what’s actually quite helpful is I tell them, “Don’t do deep pressure. Actually do something such as cupping or a technique called pressure-sage,” where you’re lifting the tissues away from the nerve. You can buy online silicone or plastic cups that are little suction cups that you put on your arm or your forearm and they’re like $3 each. You can put these little suction cups on your forearm and go through a series of glides and stretches that lift the muscle away from the nerve and decompress it. That was a technique that I utilized.
Neely Quinn: If people are going to look on Amazon for these cups, what would they look for?
Dr. Jared Vagy: Rock Tape makes some good ones and they come in a little holder or whatnot, but you can also get them from China. There’s these pink silicone cups that you can get that are only a couple bucks and you get like 20 of them. On Amazon I bought like 30 different brands of cups and I tried them all on and there’s huge inconsistency in the ones that you get. I found one that’s quite cost-effective and they’re pretty good. Let me give you a link where people can find those if they’re interested in checking those out. I’ll give you a link to attach to the podcast so people can find those cups online because they’re pretty cool.
What you do is you put them on and then you do what are called nerve glides. They are these different movements where you move your neck and move your elbow in different positions to tension and slacken the nerve, almost like you’re tensioning and slacking a climbing rope. These aren’t like stretches. You don’t hold a prolonged stretch. You almost put yourself in this owl eye position and then you move your head back and forth or you move your elbow up and down.
I think for some of this stuff, Neely, let me just give you – I have Sean McColl pictures and videos of him doing these really cool nerve glides for the ulnar nerve. Let me just attach that to this episode so people can kind of see what a nerve glide looks like. I’ll give the link to the cups as well so they can see how that process goes.
Neely Quinn: That’d be great. Cool.
Dr. Jared Vagy: That’s one thing I think I wanted to bring up, that differential of inside elbow pain, especially with climbers that have had it for a long time and it’s been persistent. Start to look to see if something else is causing it or if there’s an additional factor that’s leading to it.
Now, if it’s just straight-up inside elbow pain it’s pretty straightforward. You unload the tissues. The Rock Rehab Pyramid, as we’ve talked about in these episodes in my book, you go through and you have at the base of the pyramid ‘unload the affected tissues.’ Once you unload the tissues you increase the mobility through some stretching and then you increase the strength and then you change the movement.
If someone has inside elbow pain, Neely, on your site and they don’t have the nerve affected like I just talked about, on your site I’m going to get up some protocols so you’ll have this by the time the podcast posts where people can access where it has a very streamlined ‘How to unload the inside elbow’ with a tape job. There’s a tape job that you can basically tape to take pressure off of that tendon. Then, the mobility exercises, the stretches they can do to increase the mobility in the wrist and the fingers. The strength exercises – what’s called eccentric which we’ll talk about in a little bit – that they can do to increase the strength of the tendon and then the movement patterns and changes they can have. For inside elbow pain and outside pain, we’ll get those up on your site, something that people can go through protocols for.
Neely Quinn: Okay. Can you give an example of a couple of the eccentric strength exercises they would be doing?
Dr. Jared Vagy: Eccentric strength exercises – first of all, it’s important to know that the research on inside elbow pain and eccentric strength exercises is not as good as on outside elbow pain but still it’s important to do them and it’s common practice now to do them.
What eccentric exercise is, just to give people an idea, is basically think of your biceps muscle. You take a weight and you curl the weight upwards and that’s concentric. You slowly lower it down and that’s eccentric. You hold it in one position and that’s isometric. Those are the three terms that we’ll talk about.
For eccentric exercises for the inner elbow, one thing that most people forget is earlier we talked about the three different muscle groups that attach to the inner elbow. Should I quiz you on this, Neely?
Neely Quinn: No. [laughs]
Dr. Jared Vagy: We’ve got the professor in me coming out. [laughs] We’ve got the finger flexors, we have the wrist flexors, and we have this pronator muscle. Oftentimes, when people do eccentric exercises what they forget to include is also this pronator muscle. What I’ll have patients do, and this is in the protocol for eccentrics, is they’ll just grasp a hammer, a frying pan, a beer bottle, a wine bottle, whatever leverage that they need. They’ll have their elbow down at their side, their elbow flexed at 90°, they’ll hold this frying pan so the frying pan is facing up into the air, and then they’ll slowly rotate until their palm is facing up and the frying pan is parallel to the ground. They’ll help the frying pan back into that starting position and then slowly rotate again so their palm is facing up and the frying pan is parallel to the ground. They’ll do three sets of 15 of those daily. They’ll do that with their elbow bent but then also with their elbow straight or extended.
They’ll straighten their arm so their elbow is at the height of their shoulder, their wrist is at the level of their elbow, and they’ll basically have that frying pan, holding it straight in front of them and then rotate that frying pan so that the palm is facing up, help it back to the starting position so that they’re only working on the eccentric component, and then rotate again so the palm is facing up. Again, three sets of 15 repetitions.
Neely Quinn: Okay. That’s pretty straightforward.
Dr. Jared Vagy: Yeah, and you could do that with a resistance band, you can do that with a weight by just grabbing the edge of a weight, but I like doing it with a frying pan. Everyone has different pans. I have this really small one I like to make a single egg on, I have these large ones where when strong climbers come into the clinic, I like using a bigger pan. You can find the right resistance or adjustment.
I used to big wall climb a lot so I have a big wall hammer and I would just attach on the little keyhole – they call it a wall hammer – basically a piece of cordage and a bunch of gear. Then I would hold this hammer and just do these rotations with a hammer and a bunch of gear off of the end of it. I didn’t really cook that much and I didn’t want to use my frying pan for exercises so that was my dirtbag way that I would do it. That’s a really good way to eccentrically strengthen what’s called the pronator. That’s one of those three muscles that we talked about that can cause or generate some of that inside elbow pain.
Other ways for the wrist flexors – that’s another muscle that can cause inside elbow pain – just simply if you put a weight and you put it in your hand and you help curl that weight up. Imagine your elbow is at your side, your elbow is bent at 90°, your palm is facing up, you press your wrist into flexion or kind of press your wrist up, and then you slowly roll your wrist back and down, extending your wrist. That’s going to be your eccentric component for those wrist flexors.
Neely Quinn: And they should do all of these exercises?
Dr. Jared Vagy: Here’s the thing and this is where it becomes specialized: if you’re doing a protocol and you haven’t seen a medical professional and you’re not sure exactly which of these three muscles is generating that elbow pain, yeah, you’ve got to do all of them. You’re not sure which one it is so one of them is going to be the most likely one that’s going to help you.
If you went through those muscle tests that we talked about earlier and let’s say that we identified that, ‘Oh no! Just that finger flexion is the one that causes my pain,’ then just do the eccentrics for the finger flexors. If you realize that, ‘Oh no! Just the wrist flexion. That’s the one that causes my pain,’ do the eccentrics for the wrist flexors and if you realized that no, it was just that pronation or that rotation one, do that eccentric.
The protocols are a catchall. They allow you, if you have pain, to pretty much catch all those diagnoses. If you do the self tests or have a medical professional do the tests on you, you can probably decrease the amount of exercise you have to do to maybe only one or two in that strength category.
Neely Quinn: Did we talk about the – we talked about the wrists but we didn’t talk about the finger flexors, or am I getting that backwards?
Dr. Jared Vagy: Oh no, we did not. We talked about the pronation and that’s basically taking the frying pan and rotating that frying pan side-to-side. We talked about the wrist flexors which is just a simple exercise. You just take a weight and you can slowly lower or extend your wrist with the weight. Then the finger flexors, one that I like to do quite a bit is if you just take a barbell or even a dumbbell – you know finger roll-ups? Where you basically take a dumbbell and you flex your fingers? You rest the dumbbell on the tip of your fingers, you flex your fingers up, and then you slowly open your hand and kind of roll the dumbbell downwards.
Neely Quinn: No, I’ve never done that.
Dr. Jared Vagy: Imagine a dumbbell, or you can hold anything really with this. Let’s say you have a 25-pound dumbbell in your hand and you start with it in this closed grip but you put the dumbbell edge of the handle on the tips of your fingers and then you slowly open your hand until you almost feel like you’re going to drop the dumbbell. You can get to the lowest position until your hand is almost fully open and that’s eccentrically lengthening the finger flexors.
There are two different finger flexors. I don’t want to get too complicated but there’s flexor digitorum profundus, which is at the tip of your fingers, and superficialis which connects to right underneath the tip of your finger. If you wanted to get very fancy you can do a finger tip roll on the tips and then you could do one that’s a little bit closer to the palm. All that is is then you help it back up into the fist and then you slowly open your hand until you almost feel like you’re going to drop that dumbbell on the ground and then you help with your other hand and slowly close the fist. You repeat that same sets, same repetitions.
Neely Quinn: Okay. These are great.
Dr. Jared Vagy: The thing that I’ve found is the reason that a lot of climbers don’t do well with these elbow diagnosis is 1) they’re misdiagnosed, and we talked about that, and the other is can you imagine how many three sets of 15 – that’s 45 repetitions – and you’re doing that for three different regions? Actually, before, if you include profundus and superficialis the two finger flexors, now you’re doing 180 repetitions of an exercise every day. The compliance for that is terrible, right?
What I oftentimes recommend is self-test yourself. Make life easier. If finger flexion generates your elbow pain, just do the finger flexor eccentrics because three sets of 15, which is 45 repetitions, is plenty of exercise to do in one day.
Neely Quinn: Yeah. It’s so frustrating because I can’t even think of a physical therapist in the Boulder area who is really good with climbers. I’m sure I’m missing somebody in my head but you have such great knowledge about this. If people really don’t know how to diagnose themselves, you do remote consultations, right? Or no?
Dr. Jared Vagy: No, I do. I’m at about a 70% non-acceptance rate so I basically have to turn away about 70% right now just because of time. Here’s the thing, Neely: I think things are changing quite a bit. Every year that I get on this podcast or every year that I talk about climbing injuries or every year that goes by and something new changes or adapts, there’s more and more medical professionals that are skilled with treating climbers. It’s incredible.
We even have, when I teach at USC in the doctoral physical therapy program that we talked about earlier, a climbing special interest group. Once a month in each class – there are three years in the physical therapy curriculum. In each class there are students that join this special interest group and we sit down and I talk through with these future physical therapists and I educate them on, ‘Here’s how you diagnose and how you treat rock climbers.’
The whole point of this book that I put out, Climb Injury Free, was: can we get this knowledge and information to medical professionals that is climbing specific? There are plenty of great medical professionals, we just need to add in the climbing specificity.
I think with the protocols that you have on your site, that’s a thing as well – let’s relate this to rock climbing. I think this is changing. I’m hopeful in the next few years there’s going to be tons of local physical therapists, chiropractors, acupuncturists, whatever medical professional – people that specialize in climbing because I’ve just been seeing it more and more but that’s my bias. I’m all about education and I’m trying to get this information out to as many people as possible.
Neely Quinn: And that’s good news. That’s really good to hear, actually.
Dr. Jared Vagy: That’s my soap box on those things.
Neely Quinn: So there’s hope. People might be able to find somebody who can help them.
Dr. Jared Vagy: Yeah, you should be able to find someone and if not, let’s find some ways to self-diagnose at least, right? Find some ways like I talked about on this podcast, like if you have this injury then try that owl eye position and see if your neck movement changes. Try testing these different muscles on yourself, which you can do, and see if it generates pain and then there are some protocols that you can follow that may be able to help you. If you don’t want to get the protocols then listen in depth to this podcast and that will be able to tell you most of the stuff that’s there.
Neely Quinn: Cool. So we’ve covered most things for medial elbow pain but is there anything that you want to talk about before we move on?
Dr. Jared Vagy: No, I think we can move on from medial elbow pain.
Neely Quinn: Okay, what’s next?
Dr. Jared Vagy: Let’s talk about outside elbow pain or the lateral elbow pain.
Neely Quinn: Okay, what does that look like?
Dr. Jared Vagy: Same thing. You have pain in a specific region of your elbow. If right now you’re sitting there driving or walking or whatever you’re doing, if you rotate your palm down and trace your wrist muscles from the back of your wrist up to the outside of your elbow they attach into a little bony knob on the outside of your elbow. This is a region where oftentimes people will get a similar type of tendinopathy and it’s called lateral epicondylosis, or if it’s within the first two weeks it’s lateral epicondylitis.
This was one that for the longest time I was having trouble finding out why climbers would get this. We talked about before that we’re constantly flexing our wrists, flexing our fingers, so it makes sense that we would get inside elbow pain because those flexors are overactive. We’re overusing them but why on earth would a climber get outside elbow pain? Do you have any thoughts on that, Neely?
Neely Quinn: I mean, is it just an imbalance?
Dr. Jared Vagy: It is, yeah, it’s an imbalance and it’s something that actually has to do with how we grip. If you think about it, just kind of relax there with your wrist relaxed and flexed forward and then slowly start to extend your wrist backwards. What you should notice is as you extend your wrist backwards, your fingers will naturally start to flex in toward your palm. You kind of have your wrist dangling and then you extend your wrist backwards and your fingers will start to just naturally flex in towards your palm. Is it doing it for you?
Neely Quinn: Yep.
Dr. Jared Vagy: When I started looking at this and started going into the research, our strongest grip is when our wrist is cocked back or extended about 35° so our strongest grip is when our wrist is cocked back. If you think about when you contact a crimp on the rock wall, the geometry of our hold is we actually have to cock our wrist back to grasp it unless it’s fully overhead and we can rest our elbow against the wall but to grab on crimpers, we’re constantly cocking our wrist back in that position.
Then I started thinking: okay, if you’re constantly cocking your wrist back in that position, that’s probably why people have outside elbow pain. They’re overworking those wrist extensors to try and grip harder. They’re extending their wrist back, locking out that position, then trying to crimp down and grip. That could potentially cause that overuse. This is where I then had to say, “Okay, we know how to treat that.”
We talked about before how there’s decent literature that supports what’s called a Tyler Twist, these eccentric exercises just like we talked about for the inside elbow pain. Have you ever seen a Flex Bar? It’s this green, blue, or red rubberized bar that’s about 12” long that you twist in different positions? Have you seen one of those, Neely?
Neely Quinn: Oh yeah.
Dr. Jared Vagy: A Flex Bar is kind of a cool tool that you can use. You grasp it in your hand, you extend your wrist back, you straighten it in front of you, and if you go through this series of different exercises that eccentrically work on those extensor muscles, that’s something that you could do. You could even take weights and you could slowly lower your wrist down just like we talked about for the inside elbow pain but just the reverse. You could do these different types of eccentric strengthening exercises for that area.
What was actually fascinating was a case study that came out in JOSPT, which is a physical therapy research journal. They did this in a fellowship in southern California where a non climber came in and they had outside elbow pain, so they had lateral epicondylosis like what we’re talking about. They looked at them with their shirt off and they noticed that their shoulder blade was winging away from their body.
Imagine the shoulder blade kind of in a bad position, winging away, and this is actually quite a common finding. We don’t often see the backs of our shoulders but you can look at the backs of your friends’ shoulders and oftentimes observe this. What they did was this patient gripped a dynamometer and it told them their grip strength. They had a 4 out of 10 pain in a low grip.
The therapist then came in and they stabilized the shoulder blade.
Neely Quinn: With tape?
Dr. Jared Vagy: No, with their arm. They basically took their arm, took their hand, and did what’s called a scapular reposition test. They manually just held the shoulder blade in place and the patient squeezed on the dynamometer. Their pain was 0 and their grip strength went up.
Neely Quinn: Interesting.
Dr. Jared Vagy: Then they did a case study where they actually treated this patient. They gave them shoulder blade stabilization exercises to stabilize their shoulder blade, they gave them posture cues, they also taped them into that position of their shoulder. They did not even touch the outside of the elbow and upon follow-up, 0 out of 10 pain. They filled out these surveys or these self-report questionnaires and they’d returned to full function.
Neely Quinn: That guy was psyched.
Dr. Jared Vagy: Yeah, he was so psyched that he actually wrote a research article and got accepted into international publication so something that’s read around the world. What’s really cool about that is you’re treating the entire kinetic chain, you’re not just treating the area that’s affected. In climbing, I think that is so important.
If you think about it, when you’re gripping onto a hold, imagine if your shoulder blade is unstable. How much more do you have to grip to keep your body pinned against the wall to keep yourself from falling? When I see patients in the clinic or when I treat them, every time someone has outside or even inside elbow pain, I need to make sure that we’re addressing their shoulder blade as well and not just the symptoms on the outside of their elbow.
Neely Quinn: So it’s kind of a given that this might be part of the issue?
Dr. Jared Vagy: It’s a given that it may be part of the issue but you have to test it so I’ll do the same test. You have them grip and see if it generates pain, reposition their shoulder blade and see if it improves. You do that with their elbow down at their side and then you start doing that in climbing-specific positions. You can start doing that with their elbow a little bit higher in that position, you can have them squeezing on a squeeze ball as they start to go through different positions, reaching overhead, see the positions where they feel the most discomfort in the outside of the elbow and then reposition their scapula and see if that changes.
This is especially prevalent if somebody also has a history of shoulder pain. Oftentimes you’ll see somebody who’s like, ‘Oh, my right side. This is the shoulder that I dislocated and for some reason this right elbow is also hurting.’ This is also a sign for you to lean towards looking beyond the location of the injury.
Neely Quinn: So then they do scapula exercises?
Dr. Jared Vagy: They do scapula exercises, correct, and they do some movement retraining, teaching them how to reposition their shoulder blade when they climb. In addition, yes, we do treat the affected tissues. For outside elbow pain, the same thing: we go through this rock rehab pyramid. At the base you have pain/inflammation/tissue overload and you need to address that so I’ll typically unload that with a certain tape job that basically takes stress off of the tendon. You then improve the mobility but the mobility is a little bit different. For the mobility I actually have them release the wrist flexors so they’re going to do a lot of soft tissue massage to the muscles in the front of their wrist. Any idea why we would release the muscles in the front of their wrist to help them with overuse of the muscles in the back?
Neely Quinn: Again, probably just an imbalance, like maybe it’s pulling on the back muscles?
Dr. Jared Vagy: That’s entirely the case. Imagine if you have really tight flexors of your wrists that are flexing your wrist and fingers forward. You have to work harder to extend your wrist and fingers backwards. The soft tissue to apply is not to the affected region, it’s to the opposite side. They can take a lacrosse ball, they can use an Armaid, they can use any type of device to start to free up their wrist flexors, the muscles in the front, so that their wrist extensors, the ones in the back, don’t have to work as hard to extend their wrist back.
Neely Quinn: Very interesting. These are not things that people would think of on their own, Jared.
Dr. Jared Vagy: That may be true, that may be true, but now they know them. If they listen to this podcast they’ll have that information. ‘Oh! I have outside elbow pain. Why on earth was I massaging the outside of my elbow? I have to massage the inside and free up the opposite region and oh, by the way, I was in a push-up position and someone looked at my shoulder blades and they noticed that my right shoulder blade was winging away from my body. I’m just going to add in the shoulder blade stability exercise to stabilize the foundation so my elbow is not overworked.’
I think climbers can now think of that. Neely, we talked about how you go from this pain/inflammation/tissue overload and you go into this mobility where we talked about you’re freeing the flexors up. From mobility we go into strength. What type of strengthening exercises would we do for the outside of the elbow? It would be eccentrics, right? This kind of lengthening position.
Then we go into movement and we can change their movement patterns. Don’t overgrip, especially when you’re runout. You’re 10 feet above a bolt, 15 feet above a bolt, 20 feet above the bolt and you’re overgripping everything. Relax your nervous system. Easier said than done. You’re on your warmup. Don’t try and crush your V3 when you’re warming up. Save some power in your fingers for the crux move – those types of things – for when you get to a higher level and you’re on your V10. Those are the things to think about from that progression.
The reason for this podcast is I like to then take these protocols or take these norms – and the protocols will typically help 80% of people with this condition – and then expand it to say, “Hey, what are some other things that you can start to think about?”
Neely Quinn: It seems like there’s a lot of other things that you can think about.
Dr. Jared Vagy: Yeah, there are all of these nuances. For example, someone with outside elbow pain, it could also be the supinator muscle which is this little tiny muscle that rotates your wrist back. It could be the radial nerve which is a nerve that passes under that area. There’s all these really interesting things but we only have a certain amount of time on the podcast and I don’t want to jumble listeners’ brains with all of these things. What I’m trying to bring about is no matter what it is, I really recommend that people use a systematic approach so you know that you don’t miss anything. Pain/inflammation/tissue overload? Address that. Mobility? Address it. Strength? Address it. Movement? Now you’ve got everything covered.
Neely Quinn: Cool. So that’s outside elbow pain and then what’s next?
Dr. Jared Vagy: We have anterior elbow pain and posterior elbow pain, so front of the elbow and back of the elbow.
Neely Quinn: What does anterior elbow pain feel like? Where is that?
Dr. Jared Vagy: Normally it’s called anterior medial. It’s in the front of the elbow but slightly towards the inside. This is one that a lot of climbers get confused. They don’t know whether it’s golfer’s elbow that we talked about earlier in the podcast, this medial elbow pain, or if it’s bicipital tendinopathy, this front of the elbow pain, and it’s sometimes tough to differentiate. What I see a lot of, the movement pattern that climbers present with that have mostly this front of the elbow pain, or anterior elbow pain – are you able to guess that one at all, Neely? Think about what would overuse the muscles in the front of your arm? Those biceps. What climbing pattern?
Neely Quinn: Underclings? I’m not really sure.
Dr. Jared Vagy: For sure. You got it. Underclings are using those biceps to pull your body into the rock wall. Sometimes even sidepulls are kind of a tricky position that will overuse it a little bit. What general climbing style?
Let’s say we have two climbers. You have a climber that comes in and you watch them climb and they have this graceful style. They use their feet a lot, they stem a lot, they keep their elbows extended when they’re on overhangs. Then you have this climber and let’s say they’re on a roof problem and they’re just gorilla climbing. They’re nailing it but they’re flexing their elbows and they’re pulling their body in and they have this dynamic style where they’re using their upper body quite a bit. Which one of those do you think will tend to develop overuse injuries in the front of their elbow?
Neely Quinn: Probably the second one.
Dr. Jared Vagy: Yeah, probably the second one. They’re constantly using their biceps muscle to pull their body into the rock wall and that’s a common pattern that I’ll see. Do you think more female or male?
Neely Quinn: Probably male.
Dr. Jared Vagy: This one is more so in male climbers. I see this a lot in male climbers, ones that have the strength in their upper body, they’re going to overuse that biceps. The biceps, if you think about it, we have our brachialis, which is on the inside, and the biceps brachii is on top, but those originate in the lower arm in that elbow crease. They attach up higher into the shoulder and one of them, the long head of the biceps is actually into the shoulder blade and the short head into what is called the coracoid process. You have these biceps muscles that attach into the shoulder and then their origination is at that crease of the elbow. That constant overuse can start to lead to pain at the crease of the elbow.
Neely Quinn: So what do they do?
Dr. Jared Vagy: From the movement perspective, when they’re on an overhang. Imagine that climber is in the gym and they’re doing the roof or the overhang ceiling. They’re in that position and they’re constantly using their biceps to flex. Instead, we have them extend their elbows. The challenge with that is when you extend your elbows, what happens to your center of mass? It drops towards the ground, right? You’re completely in a roof and overhang and now you’re going to have to work harder so what you end up doing is they extend their elbows and straighten them but then they pull their shoulder blades back just a little bit. By pulling their shoulder blades back just a little bit, that brings their chest forward.
Neely Quinn: It seems like doing some core work would also help with not using your arms quite as much.
Dr. Jared Vagy: For sure, and that’s why part of these protocols, especially for elbow pain, is some core training with your elbows extended. Doing something like you’re on a squat rack and you put the bar locked into higher position, so you’re almost in a reverse push-up so your hands are hanging from the bar but your chest is facing the sky. Does that make sense?
Neely Quinn: Totally.
Dr. Jared Vagy: Then you kick your legs up on the bench and you could basically do some core work. You lift one leg, you lift the other leg, you squeeze your shoulder blades, you do all that while you are engaging your stomach, engaging your stomach, but you’re relaxing your biceps.
Neely Quinn: That’s great training for that.
Dr. Jared Vagy: If that’s too easy and you’re a hotshot and you can do that very easily, let’s put your feet or your heels on an exercise ball like a Swiss ball, so a giant blown up ball that is unstable. Now hold that position while you lift one foot up and lift one foot down from that ball.
Neely Quinn: Would front lever training do the same thing?
Dr. Jared Vagy: Front lever training for sure. If you can break down a front lever and be able to do each component of it, absolutely that’s something that can help as well. That would obviously be a higher level of training but 100% that could train it as well, as long as you’re keeping your elbows extended.
One other thing with going back to the bar is then you can even do that with one arm. Then you can imagine you’re in this reverse push-up position, you’re hanging from both arms, your feet are on an exercise ball. Hold that position then release one arm without bending your elbow. There’s a lot of progressions that you can do but you get the point with the movement.
Neely Quinn: Yeah, but when you’re on the wall, just being better about keeping your shoulder blades engaged and extending your elbows more often.
Dr. Jared Vagy: Exactly, but more so when you’re on an overhang. If you’re on vertical terrain, if you keep your elbows too straight your center of mass is going to shift down to your legs which is okay but you’re going to put a lot of weight into your fingertips. A lot of these are more movement suggestions versus movement rules. Knowing that you’ve got to bend your elbows when you climb, you’ve got to pull with your biceps, there’s a time and a place and you may potentially overdo it so just be mindful of those positions.
Neely Quinn: Okay. Then what do they do?
Dr. Jared Vagy: If you think about the Rock Rehab Pyramid we have the foundation, which is then our pain/inflammation/tissue overload. There’s not good research that supports taping or bracing for elbow or triceps tendinopathy so it’s one that I don’t include within those protocols but you get into mobility now. If you think about it, as you’re constantly flexing or overusing those biceps, we want to be able to stretch them and be able to stretch the biceps muscles out. There’s some different exercises. One I really like is that you’re on a hands and knees position and then you flip your wrists around so that your fingertips are pointing towards your knees. Can you imagine that?
Neely Quinn: Yeah. I think it’s called gorilla pose or something in yoga.
Dr. Jared Vagy: Okay. So you’re in that position and then you engage your triceps muscle. For people doing this, just make sure your biceps are tight because a lot of people have extra bend in their elbows. They hyperextend their elbows and for someone that hyperextends their elbows, this would not be recommended. If you have stiff biceps and stiff elbows, you rotate your palms around and then you can kind of sit back into that position and start to put a little bit of stretch on the tendon and the muscles in the front of your arm.
Neely Quinn: Yeah, that makes sense.
Dr. Jared Vagy: I like that too because your wrist is extended back so you also get this wrist flexor stretch which, as climbers, we need quite a bit of.
Another one is you can just stand, place your hand against the wall almost at the level of your shoulder and extend your wrist back so you’re pressing against the wall, then you just rotate your body away from your arm. That will stretch out not only your chest muscles but also the muscles in the front of your elbow, so the biceps. There’s plenty of ways to mobilize or increase the mobility of the biceps.
Then we get into strengthening. Protocols for eccentric strengthening do quite well for outside elbow pain, they do okay for inside elbow pain, but I haven’t seen good results clinically for biceps tendinopathy. I actually just have them strengthen and stabilize their shoulder blades through these positions we talked about earlier, these core positions where you’re challenging your stomach muscles but you’re keeping your elbow extended and your shoulder blades engaged.
One of these is actually quite simple. When you’re in a plank position, you just go and open up into an airplane. You basically open up into a side plank with one arm reaching up into the air and then you lower back into the plank again.
Neely Quinn: Oh, and then you can do each side at different times.
Dr. Jared Vagy: Exactly, and also your shoulder blade is engaging and stabilizing as you press into the ground to keep that elbow straight. It’s training this movement pattern of your triceps turning on, your shoulder blades turning on, your biceps turning off, as your core engages and you rotate.
Neely Quinn: Yeah, that totally makes sense.
Dr. Jared Vagy: You could do that with your knees straight but I also like to have climbers do it with their knees bent because when your knees are bent almost in this bear position, that simulates a little more of the position you’d be in on the rock wall.
Neely Quinn: Okay, so that’s strength then we can talk about movement.
Dr. Jared Vagy: It’s kind of cool. For any diagnosis, if anyone is listening and they have an injury and maybe it’s not even one that we talked about, see if you can take yourself through and do one exercise in each category. Make sure you’re not skipping a category so you’re able to fully create a treatment plan that doesn’t miss anything.
Neely Quinn: Easier said than done.
Dr. Jared Vagy: Easier said than done.
Neely Quinn: So that was anterior. Is it the same for posterior or what would you say for that?
Dr. Jared Vagy: I’d say for posterior, this is going to be more your tricipetal tendinopathy and your triceps, the muscle in the back of your upper arm as it attaches into that bone. Any idea, Neely, what movements will stress this quite a bit?
Neely Quinn: Mantles?
Dr. Jared Vagy: Mantles for sure. If there’s a route at the gym or the crag called Mantle Marathon, this may predispose you to some triceps tendinopathy.
Neely Quinn: Maybe some really deep lockoffs?
Dr. Jared Vagy: Yeah, kind of in a different way. Deep lockoffs are going to work your biceps but that’s going to compress the elbow joint so I agree, a deep lockoff can cause some elbow pain. Take that lockoff and spin that elbow up in the air and that positions you almost in a gaston. The gaston is going to put quite a bit of strain on the triceps, especially because now that’s a position that your shoulder blade has to work even more.
Neely Quinn: Oh, I see. That makes sense.
Dr. Jared Vagy: Those are all potential ways that can develop some tendinopathy if you’re overusing those positions or if you’re in a crux and you push really hard and you strain the muscle when you’re doing that. Then you can go through a similar thought progression. Pain/inflammation/tissue overload – there’s not great research on taping to support it so you just kind of wait those two weeks and kind of slowly regain your motion. Mobility – this one I have climbers just take a piece of cordage from their crag bag and bring their elbows up to the shoulder height, grab the piece of webbing or tubular webbing or whatever you have in your bag. Grab your climbing rope if you need, and then you just extend and straighten one elbow as you flex the other. Extend and straighten your other elbow as you flex the other and just basically go back and forth, straightening and extending your elbow with a very mild amount of resistance that you’re applying on the rope.
It’s a way to mobilize the area but at the same time create a little bit of muscle tone to resist the motion as well.
Neely Quinn: Okay, that makes sense.
Dr. Jared Vagy: Eccentric exercises – let’s say that’s one in mobility and then we move up to strength so now we’re at the strength level of the pyramid. There are a bunch of ways to do eccentrics. If your issue is mantling, that’s a closed-connection exercise. You can do some unweighted mantles, basically having yourself in that position, going through a partial range dip. I’m not excited about dips in general because they put a lot of stress on the anterior aspect or the front of the shoulder but there are some modified ways that you could do that.
The go-to that I have for this is actually quite a simple exercise where you’re doing almost a tricep press in the gym. You have resistance and you’re pressing your arms down and straightening your elbow to turn on that triceps muscle. Doing that but doing it with a resistance band so you take a resistance band and you kneel on the ground. I like the kneeling or squatting positions because it’s going to simulate the bend in your lower body when you climb. So you’re squatting or kneeling on the ground, you grab the resistance band with one arm, your non-injured arm, and you raise that above your head. You then grab the other end of the resistance band with your injured arm and you bring it out to your side then you press your injured arm straight into that triceps position, that fully extended arm position, and you slowly let it come back down to the start position. You press it straight then you slowly let it bend back to the start.
Neely Quinn: Could you attach the band to something so that you don’t have to hold it?
Dr. Jared Vagy: You could but why do you think I like climbers to hold it with the other arm?
Neely Quinn: Um…
Dr. Jared Vagy: Think about climbing movement and what we do.
Neely Quinn: Yeah, I mean I guess we’re always using both of our arms.
Dr. Jared Vagy: In climbing movement you’re stabilizing with one side and then you’re moving the other. I actually like that one quite a bit. They have to work a little bit in that opposite arm and in their shoulder blade to isometrically stabilize as they’re going through this exercise that’s moving the opposite arm. Since one arm is reached over your head, the other arm is down and now we’re starting to simulate what the body does when we climb.
Neely Quinn: That makes sense.
Dr. Jared Vagy: Of course we could attach it to the wall. We could do two arms at once and that will probably address the same goal but my mind is always thinking, ‘How can we make this a little bit closer to climbing? Can the climber squat down? Can they put one arm in the air? Can they start to simulate those movements a little bit more closely?’
I think those are the four common places that people would have pain in their elbow. I’m hoping a little bit of a taste of maybe some differential diagnoses of, ‘What if it really isn’t that?’ and then some protocols. Some ways that climbers can say, “Alright, I have pain in this area or I’m afraid of getting pain in this area. What can I do to prevent it?”
Neely Quinn: I think this will be helpful for people to at least pinpoint what they have going on and then give them some direction to try to figure out how to fix it. The protocol will be on TrainingBeta and it will be with the rest of the Rock Rehab Pyramid protocols and they’re pretty awesome and very affordable. Also, I’m assuming that a lot of the things we just talked about are in your book as well.
Dr. Jared Vagy: Yeah, almost all the things we discussed, and even the nerve glides as well, those are in the book Climb Injury Free. I’m psyched on the book. It’s gotten really good response from the climbing community and it’s helping a lot of people. I can only do so much so my goal is to try and get as much content out there in a variety of forms that people can be psyched on so that info is also in the book.
Neely Quinn: Which is called Climb Injury Free.
Dr. Jared Vagy: Yep.
Neely Quinn: Cool. Did we miss anything?
Dr. Jared Vagy: No, I think we covered everything. We got inside elbow pain, outside elbow pain, anterior and posterior, and maybe the last thing I have to ask you is a quiz of 10 questions. Right Neely?
Neely Quinn: Oh god. Okay.
Dr. Jared Vagy: [laughs] I’m just kidding.
Neely Quinn: Okay, good. [laughs] This one is a little foreign to me, I will admit.
vYeah, you’ve dealt mostly with shoulder. Are there other regions you’ve had pain in your body?
Neely Quinn: Yeah, hip. Let’s do a hip one.
Dr. Jared Vagy: Oh yeah. We haven’t done a hip one yet, have we?
Neely Quinn: I think more people’s hips hurt than we hear about. It’s one of those things where my hip hurts pretty much all the time but I just ignore it because it’s pretty easy to climb through it and I think a lot of people probably feel the same way.
Dr. Jared Vagy: It’s so common. I give a lot of these different workshops and clinics and I may have mentioned this in a previous podcast but I see a lot of climbers with upper body injury and I don’t see that many or they don’t come to see me with lower body. Then I go and poll coaches, climbers, medical professionals that climb, and ask them, “Alright. Who here has knee pain? Who here has hip pain? How many of you have that while you climb?” A lot of us do and it’s something that’s not talked about as much. It definitely affects how you climb quite a bit, especially with the hip if you can’t get your hip in certain positions, so that may be a fun one to go through at some point.
Neely Quinn: Yeah, super fun. It’s super fun. [laughs]
Dr. Jared Vagy: Fun for me and hopefully fun for everyone listening. It’ll be educational for you as well.
Neely Quinn: Speaking of fun, have some fun in Las Vegas. I hope you have good weather.
Dr. Jared Vagy: The weather is looking great. I’m psyched and we were talking before the podcast and I think I’m going to get another long sleeve shirt to protect my elbows from some of these heinous offwidths.
Neely Quinn: Right. Just wear three shirts.
Dr. Jared Vagy: Three layers of shirts and then maybe I’ll have to grab some knee pads or something or just take the hit. This stuff used to be fun. You know, you have different types of fun. I used to be so psyched to go and do offwidths just because I would get nauseous, my body would be destroyed, I couldn’t walk afterwards, and now I’m getting a little bit older and I’m not as excited to do it but I still have a little bit of an itch. I still like torturing myself a bit and seeing if I still have it.
Neely Quinn: Yeah, it’s good for your soul, right? To be tortured a little bit.
Dr. Jared Vagy: It’s good for your soul.
It’s a pleasure talking to you, Neely, and I’m hoping listeners, especially ones with elbow pain, are able to take away from this episode some useful things to do on their own.
Neely Quinn: Thank you as always for your wisdom and I’ll talk to you soon.
Dr. Jared Vagy: Absolutely. Take care.
Neely Quinn: I hope you enjoyed that interview with Doctor Jared Vagy. He’s always fun to talk to. It’s like being in a university classroom setting when I’m talking to him. I have to really be on top of my stuff. You can find the new protocols, like I said, on trainingbeta.com/rock-rehab or just go to the ‘Programs’ page on TrainingBeta and scroll down pretty far at the bottom and you’ll find them all there.
You can find him on Instagram @theclimbingdoctor and then his website is theclimbingdoctor.com. This is a lot of information for you to remember. He also wrote a book that I think we mentioned in the interview a little bit. It’s really detailed and there’s tons of really beautiful photos in there and there are some videos that go along with it. It’s really helpful for all kinds of injuries. That’s Climb Injury Free and you can find that on Amazon or on his website or on our website.
He’s done a lot of really great work for climbers and I really appreciate the fact that he’s so willing to give this information to us freely on the podcast and then just make it available to us everywhere. That’s Jared. Please tell your friends who have elbow injuries about this podcast.
Coming up on the podcast I interviewed James Lucas. He recently got a lot better at bouldering. I asked for people to contact me a couple episodes ago. I asked for boulderers to contact me if they’ve had some really good success with training and James Lucas’s story is a little bit different. He didn’t go the standard training route with things but he got a lot better at bouldering outside and I thought it was super impressive and I loved our conversation. That will come out in a week or so.
Today I get to interview two of the guys from Elemental Gym and also climbstrong.com, which is also Steve Bechtel’s stuff. Charlie Manganiello and Alex Bridgewater both work with Steve Bechtel at his gym and on ClimbStrong and I’m going to talk to them today about what people typically do wrong with their climbing training. That’ll be interesting. Stay tuned for that.
As always, we have climbing training programs for you made by climbing trainers. You can find those at trainingbeta.com/programs and we have everything from just finger training programs to power endurance programs to an all-encompassing program for boulderers and then one for route climbers. They’re all really affordable, they’re all really step-by-step instructions. That’s what I wanted out of this site, to make things easy for people. Those are all at trainingbeta.com.
Thanks very much for listening. One last thing – you can follow us on Instagram and on Facebook @trainingbeta and then also we have a Facebook group that is getting wildly popular. It’s almost got 10,000 people in it now and everybody is just talking about climbing training, which I think is amazing that there are that many people that want to talk about training on Facebook. It’s crazy and really cool because people are giving great advice to each other. You can find that at trainingbeta.com/community or you can just go to Facebook, find our page, and then it’ll be up there as a group.
That is all now. Thank you very much for listening all the way to the end. I really appreciate you and I’ll talk to you soon.
[music]



I’m hoping Dr Vagy will provide the links mentioned in the episode. This one is particularly interesting to me.
Jeremy E Brown – I just put up some of the links he mentioned. If you scroll down the page a bit you’ll find them. Thanks for listening and let me knwo if you need anything else!